The endothelium is an organ widely distributed throughout the organism, with an approximate weight of 1.5 kg, it is deeply involved in multiple functions synthesizing, metabolizing and releasing a number of substances that exercise effects acting in autocrine, paracrine, or epicrine modes. (Bassenge, 1996). Amongst these substances the NO is of utmost importance, because of its fundamental role in several endothelial functions, such as the regulation of the vessel-motor tone, the inhibition of platelets activity, the keeping of the balance between the processes of thrombosis and fibrinosis and the regulation of the recruitment of inflammatory cells inside the vascular wall (Vallance and Collier, 1994; Court et al. 2002).
As explained, the NO and other endothelial factors are continuously synthesized and released at a level called “basic”; additionally can be released in greater amounts as consequence of the action of local or circulating ‘triggers’ (bradikine, serotonine, norepinefrine), through a process of biochemical and endocrine communication; additionally the endothelium responds to hemodynamic signals, as the increase of rub stress produced by the rise in the blood flow speed; this effect is observed, for example, during the performance of exercise, inducing acute and chronic changes in the production and release of NO (Lamontagne et al. 1992; Nishida et al. 1992), that we shall discuss further on.
The alteration of endothelium normal function has been denominated ‘endothelial dysfunction’ and is clearly associated with arterial hypertension and atherosclerosis, and has been implicated in other pathologies such as myocardial ischemia in patients with stable coronary disease, in the unstable coronary syndrome (López-Jaramillo et al. 1995), and in diabetes mellitus (Wu et al. 1995). It has been also demonstrated that, in absence of intact endothelial function, or even during normal aging process, the capacity of synthesizing and releasing NO and other endothelial autacoids is reduced, and in consequence the capacity of vessel dilation in the arteries is diminished.
It is known that blood pressure increase, whether acute or chronic produce, amongst other: endothelial damage an morphological changes in the arterial inside (Luscher and Noll, 1995); during chronic hypertension the endothelium grows into the light and the subendothelial space thickens. This might cause the reduction of access to the derivate NO from the endothelium to the flat vessel muscle, which might, in time, cause greater hypertrophy and hypertension (Berrazueta, 1995). Whether the endothelial damage is a primary or secondary phenomenon, it is clear that it aggravates the vessel anomalies and contributes distinctively in the pathogenesis of hypertension.
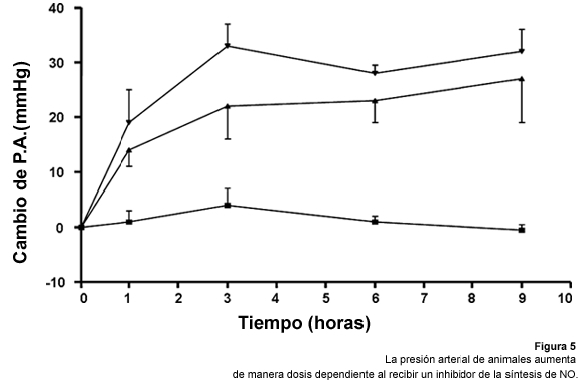
Experiments in which the interference with the synthesis or action of the NO will cause an increase of blood pressure in animals (Breslow et al. 1993; Brady et al. 2002) or in humans (Gardiner et al. 1990; Vallance, 1998; Huynh and Tayek, 2002) are already classic. The chronic inhibition of NO production will quickly conduce to all the organic consequences of a severe arterial hypertension, with atherosclerosis and loss of vessels in the Central Nervous Sysistem and kidneys (Moncada et al. 1991; Calver et al. 1993; Moncada and Higgs, 1993).
Clinically it has been demonstrated that there are lower levels of NO in patients with normal tension that are children of hypertensive individuals (Taddei et al. 1996). This suggest that some step of the synthesis and release process of the NO would be genetically regulated, explaining the cause of greater cardiac risk in patients with family hypertension. On the other hand, arterial hypertension it is associated with other risk factors, such as dyslipidemia (MacMahon et al. 1985), hyperinsulinemia (Hanson et al. 2002) and sensibility to salt (Weinberger, 1991).
t is important to point out that most of the risk factors, like the abovementioned , produce no singular symptoms amongst the patients that suffer them, which make their early diagnose difficult. This is why it is necessary to inform and educate the general population about the importance of prevention, early detection and suitable treatment of the risk factors that have a role in developing a cardiac or metabolic disease. With this aim, amongst others, the ‘Center for early detection and treatment of silent factors of cardiovascular and metabolic disease’ (SIL-DETECT) at the clinical pharmacology unit, in the pharmacy faculty, at the Universidad Central de Venezuela. Amongst the objectives of the study, it is to determine the proportion of patients which arterial pressure suffers changes according to their intake of salt (salt sensibility) in a population of apparently healthy Venezuelan adults, and study, in those patients, the possible connection between salt sensibility and the production of NO. The results of this study will be addressed further on.
Blood pressure shifting in connection with salt intake: the role of NO
The direct relationship between salt consumption, increase of blood pressure and cardiovascular disease risk has been known for over half a century (Dahl, 1957; Dahl, 1960). Different epidemiologic studies have compared the systolic blood pressure levels in populations with high and low intakes of salt. The results have demonstrated that there is a higher incidence of arterial hypertension, and cardiovascular mortality in populations which consume high amounts of salt (Page et al. 1974; Stamler et al. 1978; MacMahon et al. 1990).
Several studies of migration support those results. For example, patients coming from populations with traditionally low salt diets experimented a significative increase in their tension figures when migrating to urban zones where their intake of salt was greater and comparable to that of the western countries (Forte et al. 1989: Carvalho et al. 1989).
Nearly a 50% of arterial hypertension patients and a 30% of the patients with normal tension, appear to be sensitive to the shiftings in the intake of salt (or ‘salt sensitive’). This sensibility appears as medium blood pressure rise of 10 mm Hg throughout a diet of salt of 200mEq/d (high salt) en comparison to their medium blood pressure during a diet of only 10-20 mEq/d (low salt). On the other hand, it is considered that a patient is ‘salt resistant’ when his middle blood pressure shifts less than 3mmHg when under a high salt diet, as the aforementioned (Campese, 1994; Morimoto et al. 1997). It is a fact that, in comparison with hypertensive salt resistant patients, the patients with hypertension and salt sensibility support greater increases in their blood pressure over the years (Weinberger et al. 1991), have a greater incidence of left ventricular hypertrophy and microalbuminuria (Bigazzi et al. 1994; Morimoto et al. 1997).
In spite of the interest in the area and its clinical importance, there is still no certainty about the determining factors of salt sensibility in humans and the implications of NO in the appearance of it. Some studies performed on animals have been published in which was demonstrated that NO plays an important role in the control of the excretion of sodium and nephric hemodynamic (Ikenaka et al. 1993; Patel et al. 1994; Bech et al. 1998). For example, in obese rats, there had been demonstrated a rise in NO levels in the medulla of the kidney when increasing the pressure of nephric perfusion. They concluded that those NO increases allow the elimination of sodium without important arterial blood pressure shifts. This would be one of the motifs why the animals produce lesser amounts of medullar NO, which may be responsible for their sensibility to salt. At the same time, the rats strengthened their resistance to insulin after being treated with troglitazone. This improvement come with decrease of blood pressure and salt sensibility, and by the rise in the production of NO in the nephric medulla (Fujiwara et al. 1998). Other groups had already demonstrated that L-arginine administration on salt sensitive rats prevents the development of arterial hypertension and reduces the hypertensive response to salt (Chen and Sanders, 1991; Patel et al. 1994)
This experimental evidence indicates that an altered production of NO may be associated with salt sensibility, which is why at SIL-DETECT we evaluate the effect of high and low sodium diets over the endogenous production of NO in both salt sensitive and salt resistant patients (Cubeddu et al, 2000). In that study 89 apparently healthy patients were included, and they were evaluated in their salt sensibility and the excretion of NO metabolites. Once the salt sensibility test was performed from the total a number of salt resistant (N=25)and a number of salt sensitive (N=23) patients was selected.
Determination of salt sensibility:
The patients were under a seven day intake of high sodium (200mEq/day). During the following seven days, they followed a diet highly restricted in sodium (20-40mEq/day).
Before starting the diet and in the seventh day of both diets, the patients went back to the Center for the following procedures: measurement of systolic blood pressure, measurement of diastolic blood pressure, heart frequency, 24-hour urine for quantification of nitrates and nitrites and urinary creatinine. The following of the high or low intake was checked by quantifying the urinary sodium at the end of every seven day period.
According to the changes in blood pressure figures obtained after the high or restrictive intake of salt, the patients were classified as salt sensitive or salt resistant, in terms with the abovementioned criteria. Of the studied population 23 resulted salt sensitive and 25 resulted salt resistant. The rest of the patients were classified as salt intermediate, with shifts in their blood pressure that oscillated between 4 and 9mmHg, when changing from a high salt to a low salt diet.
|